QT Interval
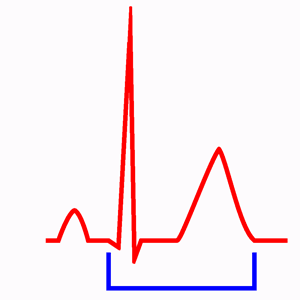
The QT interval is measured from the beginning of the QRS complex to the end of the T wave. It represents the duration of ventricular electrical systole (ventricular depolarisation and repolarisation).
The QT interval includes the QRS interval, the ST-segment and the T wave.
The U wave must be excluded from the QT interval measurement. Inclusion of such U waves can easily “inflate” the QTc by 80–200 ms and unnecessarily precipitate a diagnosis of long QT syndrome 1.
Corrected QT
See also: Corrected QT calculator
The QT interval varies depending on hear rate, it decreases at faster heart rates and it lengthens at slower rates, so to determine whether is normal or not it should undergo adequate rate correction (corrected QT or QTc).
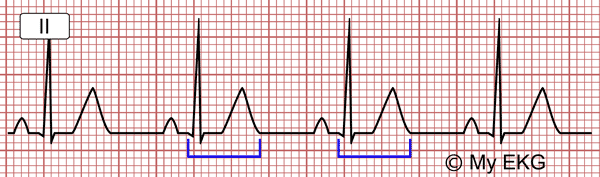
Normal QT interval: QT interval 380 ms, corrected QT interval 425 ms with HR of 75 bpm.
Of the many formulae proposed to describe this relation, the most widely used formula for correcting the rate is that of Bazett 2. But with this formula, there is an overcorrection at high heart rates and undercorrection at lower heart rates 3.
Formulae Used to Estimate QTc
- 1. Bazett formula 4: QTc = QT / √RR.
- 2. Fridericia formula 5: QTc = QT / RR1/3
- 3. Framingham formula 6: QTc = QT + 0.154 (1 − RR)
Fredericia or Framingham corrections may have more uniform correction over a wide range of heart rate. When heart rate is particularly fast or slow Fredericia or Framingham corrections are more accurate and should be used instead 3.
See also: Corrected QT calculator
QT Interval Prolongation
QTc interval is pathological if it is greater than 440 ms in men, and 460 ms in women.
QT prolongation is associated with a risk for cardiac arrhythmias given that it can result in early afterdepolarizations, provoke torsades de pointes, and lead to ventricular fibrillation, causing sudden cardiac death 3.
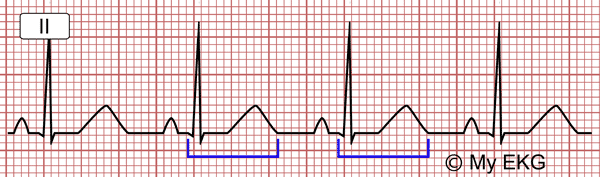
Long QT interval: QT interval 480 ms, corrected QT interval 537 ms with HR of 75 bpm.
QT prolongation can be due to common genetic variants or the acquired long QT syndrome. Acquired QT prolongation is more prevalent than the congenital form 7.
Causes of QT Prolongation
- Congenital long QT syndrome (LQTS):
- Romano-Ward syndrome.
- Jervell and Lange-Nielsen syndrome.
- Acquired QT interval prolongation:
Drugs are one of the most common causes of acquired QT prolongation 7.
More than 50 medicines have been found to cause QT prolongations. Some common medicines that may cause the disorder include: antihistamines and decongestants, diuretics, antibiotics, antiarrhythmic drugs, antiparasitic such as hydroxychloroquine, antidepressant and antipsychotic medicines, cholesterol-lowering medicines and some diabetes medicines.
Short QT Interval
A QTc interval less than 350 ms is usually accepted as pathological.
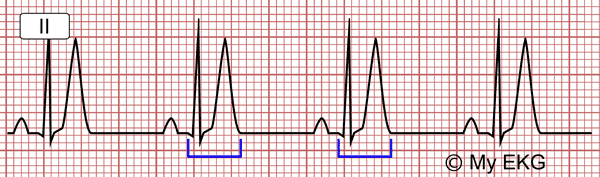
Short QT interval: QT interval 280 ms, corrected QT interval 313 ms with HR of 75 bpm.
Causes of a Short QT
Congenital Short QT Syndrome (SQTS)
Gussak et al. (2000) were the first to describe an idiopathic short QT interval as a new clinical syndrome 8.
Short QT syndrome (SQTS) is an inherited cardiac channelopathy characterized by an abnormally short QT interval and increased risk for atrial and ventricular arrhythmias.
Diagnosis is based on the evaluation of symptoms (syncope or cardiac arrest), family history and electrocardiogram findings. Implantable cardioverter defibrillator (ICD) is the first-line therapy in affected patients.
Hypercalcemia
The QTc interval is inversely proportional to the serum calcium level up to 16 mg/dL. In hypercalcemia, the ST segment is short and the duration of the QTc is decreased.
Hyperkalemia
In patients with mild or moderate hyperkalemia QT interval may be shortened, with a progressive increase in the amplitude of the T wave.
Digoxin
Treatment with digoxin frequently causes changes in ST segment and T wave. It may also cause short QT interval and PR interval prolongation.
Other Causes
A shorter than usual QT interval has been reported in patients with chronic fatigue syndrome and in response to atropine, catecholamine and hyperthermia 10.
We hope we have been able to help you with this article on QT interval. For further details on how to determine the electrical axis, click next.
previous | next
References
- 1. Surawicz B, Knilans TK. Chou’s electrocardiography in clinical practice, 6th ed. Philadelphia: Elservier; 2008.
- 2. Vandenberk B, Vandael E. Which QT Correction Formulae to Use for QT Monitoring? JAHA 2016; 5: e003264. doi: 10.1161/JAHA.116.003264
- 3. Johnson JN, Ackerman MJ. QTc: how long is too long? Br J Sports Med. 2009; 43(9): 657–662. doi: 10.1136/bjsm.2008.054734
- 4. Bazett HC. An analysis of the time relations of the electrocardiograms. Heart. 1920; 7: 353–370. doi: 10.1111/j.1542-474X.1997.tb00325.x
- 5. Fridericia LS. Die systolendauer im elektrokardiogramm bei normalen menschen und bei herzkranken. Acta Med Scand. 1920; 53: 469–486. doi: https://doi.org/10.1046/j.1542-474X.2003.08413.x
- 6. Sagie A, Larson MG, Goldberg RJ et al. An improved method for adjusting the QT interval for heart rate (the Framingham Heart Study). Am J Cardiol. 1992; 70: 797–801. doi: 10.1016/0002-9149(92)90562-d
- 7. Van Noord Ch, Eijgelsheim M, Stricker BHCh. Drug- and non-drug-associated QT interval prolongation. Br J Clin Pharmacol. 2010; 70(1): 16–23. doi: 10.1111/j.1365-2125.2010.03660.x
- 8. Gussak I, Brugada P, Brugada J, et al. Idiopathic short QT interval: a new clinical syndrome? Cardiology. 2000; 94: 99–102. doi: 10.1159/000047299
- 9. Rudic B, Schimpf R, Borggrefe M. Short QT Syndrome – Review of Diagnosis and Treatment. Arrhythm Electrophysiol Rev. 2014; 3(2): 76–79. doi: 10.15420/aer.2014.3.2.76
- 10. Bjerregaard P, Nallapaneni H, Gussak I. Short QT interval in clinical practice. Journal of Electrocardiology. 2010; 43(5): 390-395. doi: 10.1016/j.jelectrocard.2010.06.004
If you Like it... Share it.