Tetralogy of Fallot on the Electrocardiogram
Authors: Eduardo Consuegra Llapur, Ernesto C. Amalfi Aguilera.
The tetralogy of Fallot (TOF) was described in 1888 by the French doctor Étienne-Louis Arthur Fallot, after whom it is named, whereas some other authors could describe it before.
It is the most common cyanotic congenital heart disease after the first week of life, the prevalence of TOF in the United States is approximately 4 to 5 per 10,000 live births 1 2 3.
Risk Factors of Tetralogy of Fallot
Factors that increase the risk of developing this congenital heart defect during pregnancy include:
- Diabetes mellitus.
- A mother older than age 40.
- Maternal alcoholism.
- Poor nutrition during pregnancy.
TOF is also associated with other congenital disorder such as trisomies of chromosome 21 (Down syndrome), chromosome 18 (Edwards syndrome) 4 or chromosome 13 (Patau syndrome). It is also associated with DiGeorge and Alagille syndromes.
Components of the Tetralogy of Fallot
The tetralogy of Fallot includes three anatomical components (right ventricular outflow tract obstruction, intraventricular communication and overriding of the aorta), and the right ventricular hypertrophy which is the physiological consequence right ventricular outflow tract obstruction caused by the pulmonary stenosis.
- Right ventricular outflow tract obstruction or pulmonary stenosis.
- Intraventricular communication.
- Deviation of the origin of the aorta to the right (overriding of the aorta).
- Concentric right ventricular hypertrophy.
Pathophysiology of the Tetralogy of Fallot
The pressure in the right ventricle is higher than in the left ventricle due to the pulmonary stenosis.
This causes a right to left shunt, in which blood flows from the right ventricle into the left ventricle through the ventricular septal defect.
The blood with low oxygen concentration from the right ventricle mixes with the oxygen-rich blood of the left ventricle. This mixed blood is sent to the systemic circulation, causing cyanosis.
The severity of the pulmonary stenosis will be directly proportional to the magnitude of the right to left shunt and the cyanosis, and it is inversely proportional to the pulmonary blood flow.
Electrocardiogram of the Tetralogy of Fallot
In the newborn, the EKG may be normal but over the first weeks of life normal regression of right ventricular preponderance is not seen 5.
Right ventricular hypertrophy is the hallmark EKG finding in the patient with tetralogy of Fallot and is of value in the differential diagnosis from ventricular septal defect 5.
Tall R waves in the right precordial leads (V1-V2) are usually seen.
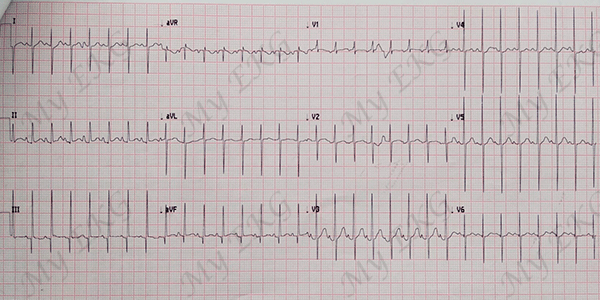
5 days old patient with Tetralogy of Fallot:
Tall R waves in leads V1 and V2 with sudden transition (deep S waves) in lead V2. Tall P wave and normal heart axis, approximately 100º.
Right-axis deviation may accompany right ventricular hypertrophy, additionally, right atrial enlargement is manifested by tall P waves (P pulmonale).
Left-axis deviation suggests an associated complete AV canal.
Sudden transition of the QRS complex morphology in leads V1 and V2 is a common pattern in patients with tetralogy of Fallot. There is a Rs pattern with a tall R wave in lead V1, and a rS pattern from leads V2 or V3 to lead V6 6.
References
- 1. Reller MD, Strickland MJ et al. Prevalence of congenital heart defects in metropolitan Atlanta, 1998-2005. J Pediatr. 2008 Dec;153(6):807-13. doi: 10.1016/j.jpeds.2008.05.059.
- 2. Centers for Disease Control and Prevention (CDC). Improved national prevalence estimates for 18 selected major birth defects--United States, 1999-2001. MMWR Morb Mortal Wkly Rep. 2006 Jan 6;54(51):1301-5.
- 3. Allen HD, Gutgesell HP, Clark EB, Dricoll DJ: Moss and Adam’s Heart Disease and Infants, Children and Adolescents Incluiding the Fetus and Young Adult, 6th ed. Philadelphia, PA, Lippincott Williams & Wilkins, 2001.
- 4. Pérez Aytés A, Trisomía 18 (síndrome de Edwards). Protoc diagn ter pediatr. 2010;1:96-100.
- 5. Surawicz B, Knilans TK. Chou’s electrocardiography in clinical practice, 6th ed. Philadelphia: Elservier; 2008.
- 6. Rijnbeek PR, Witsenburg M et al. New normal limits for the paediatric electrocardiogram. Eur Heart J. 2001 Apr;22(8):702-11. doi: 10.1053/euhj.2000.2399
If you Like it... Share it.




