Abnormal Waves and Intervals
We have followed a step by step process of determining rhythm and heart rate, whether PR and QT intervals are normal and dismissing ST segment abnormalities. Our last step is to describe any disorder not included in the aforementioned list.
For example, peaked P waves, bundle branch blocks, pathological Q waves, or negative T waves.
We recommend you to follow a simple methodology to avoid overlooking any detail, and that is, wave by wave analysis. It may seem cumbersome, but with some experience you will be able to tell at a glance if an electrocardiogram is normal or not.
Let’s make a short summary of disorders you can come upon. We remind you that the normal characteristics of EKG waves and Intervals are described in their own sections in electrocardiogram basic principles.
P Wave
Right Atrial Enlargement:
Related article: Right atrial enlargement.
It is characterized by a tall, peaked and narrow P wave (greater than 2.5 mm and less than 120 ms). This P wave is often called P pulmonale. In lead V1, where P wave is normally biphasic, the initial positive component of the P wave is prominent in V1 (greater than 1.5 mm).
Left Atrial Enlargement:
Related article: Left atrial enlargement.
It is characterized by a wide and notched P wave shaped like the letter “m”, This P wave is often called P mitrale. Lead V1 shows a deep terminal negative component.
Biatrial Enlargement:
It shows signs of both left and right atrial enlargement. Wide (>2.5 mm) and enlarged P wave. Lead V1 shows biphasic P wave with prominent initial deflection (>1.5 mm) and deep terminal deflection (>1 mm).
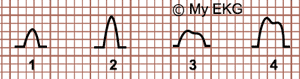
P Wave, Atrial enlargement
1- Normal P wave. 2- Right atrial enlargement.
3- Left atrial enlargement. 4- Biatrial enlargement.
Interatrial Block
Related article: Bayés syndrome and interatrial blocks.
Interatrial blocks can be classified as partial or advance block. In both blocks there is an increase in P wave duration ≥ 120 ms (wide P wave).
In partial interatrial block P wave is usually notched in leads I, II, III and aVF; whereas in advanced interatrial block P wave is biphasic (positive-negative) in inferior leads (II, III, aVF).
Both types of interatrial blocks are frequently associated to left atrial enlargement.
Ectopic P Wave:
When the initial stimulus is generated outside of the sinus node it is called atrial ectopy. If these stimuli are isolated they are called premature atrial complexes; ectopic atrial rhythm ocurrs when the ectopic focus take over the normal activity of the sinus node.
Ectopic P waves have a different morphology and axis to the sinus P waves, they are negative in leads where sinus P waves are positive (inferior, lateral or precordial leads). If the ectopic focus is close to the AV node it may produce a short PR interval.
In children may appear frequent premature atrial complexes, or even sinus P waves alternating with ectopic P waves (wandering atrial pacemaker). See pediatric electrocardiogram.
Atrial Flutter:
Related article: Atrial flutter.
In atrial flutter there are no existing P waves, normal sinus activity is replaced by a macro-reentry circuit macro-reentry circuit in the atria.
This activity causes F waves, also called “saw-tooth” waves due to the morphology in leads where they are negative.
Q Wave
Related article: The Q wave.
A pathological Q wave often appears during the natural evolution of STEMI and is associated with infarction or necrosis of the affected areas. Q waves are considered pathological when:
- They are wider than 0.04 s, deeper than 2 mm and more than 25% of depth of R wave in leads I, aVF and aVL.
- They are wider than 0.04 s, deeper than 2 mm and more than 15% of depth of R wave in leads V4, V5, V6, and aVF.
- They are seen in V1-V3 (they do not appear under normal circumstances) 1 2.
In leads III and aVF, Q wave duration is occasionally as long as 0.04 s in healthy hearts 2.
More information: The Q wave.
QRS Complex
Among QRS complex abnormalities, the most frequent are the bundle branch blocks, which widens the QRS complex.
Right bundle branch blocks: broad QRS complex (>120 ms), rSR’ pattern in leads V1-V2 and qRS pattern in lead V6. Negative T wave in lead V1 and positive T wave in lead V6. Read more...
- Incomplete right bundle branch block: narrow QRS complex (<120 ms), RSR’ pattern in leads V1-V2. Read more...
Left bundle branch block: broad QRS complex (>120 ms), QS’ or rS pattern in lead V1, and tall, notched R waves in lead V6, and negative T waves in V5-V6. Read more...
Left fascicular blocks: they do not cause widening of the QRS complex. They manifest on an EKG by axis deviations, to the left in left anterior fascicular block, and to the right in left posterior fascicular block. Read more...




