EKG Criteria for Ventricular Tachycardia
Whenever we have a wide QRS complex tachycardia on an electrocardiogram, we must assume by default that it is a ventricular tachycardia, although this is not always true.
In certain cardiac alterations, wide QRS complex tachycardias of another etiology can be observed. For example, supraventricular tachycardia with a bundle branch block or aberrant conduction, or antidromic tachycardia secondary to accessory pathway.
As you can imagine, the rapid and accurate diagnosis of an electrocardiogram with ventricular tachycardia is vital. For this purpose, we offer you some criteria for its diagnosis.
Always remember that ventricular tachycardia is the most common cause of wide QRS complex tachycardia.
Wellens Morphology Criteria for VT
In 1978, Wellens et al 1 proposed the so-called “classical criteria” to help in the differential diagnosis of supraventricular tachycardia with wide QRS complex and ventricular tachycardia.
If a wide QRS complex tachycardia presents one of these morphological criteria, it is more likely to be ventricular tachycardia.
- Atrioventricular dissociation.
- Captures or fusion beats.
- Concordant pattern: QRS complexes entirely upright or entirely inverted on precordial leads, from V1 to V6 1.
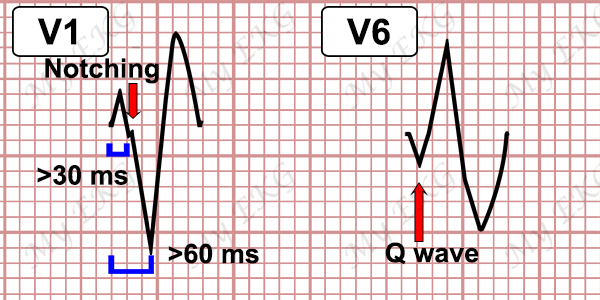
VT Criteria with LBBB-pattern
- QRS complex >160 ms and right axis deviation.
- In leads V1-V2: initial and wide r wave (>30 ms), slurring or notching of the downstroke of the S wave. Duration from the beginning of the QRS to the nadir of the S wave greater than 60 ms.
- In lead V6: presence of initial Q wave (qR) or QS morphology.
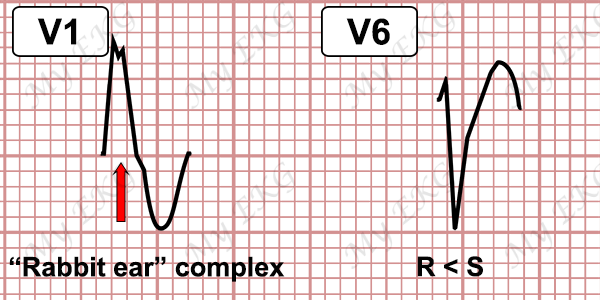
VT Criteria with RBBB-pattern
- QRS complex >140 ms and left axis deviation.
- In leads V1-V2: qR complex, monophasic R wave complex, or “rabbit ear” complex (RR') with R wave wider than R'.
- In lead V6: R wave smaller than S wave, or a QS complex.
Brugada Criteria for Ventricular Tachycardia
These criteria for ventricular tachycardia were described by Dr. Brugada et al in 1991 2. If any of them are fulfilled, you are faced with a ventricular tachycardia, if none are fulfilled, it is probably a supraventricular tachycardia.
Brugada Algorithm for Ventricular Tachycardia
It is a ventricular tachycardia if there is:
- Absence of an RS complex in all precordial leads.
- R to S interval greater than 100 ms in one precordial lead.
- If there is atrioventricular dissociation.
- If the morphological criteria for ventricular tachycardia are present both in precordial leads V1-V2 or V6 (see above).
If none of the previous statements are fulfilled: It is a supraventricular tachycardia.
Vereckei Criteria for Ventricular Tachycardia
In 2008, a new algorithm has been proposed by Vereckei et al. 3 4, these criteria are focused on the aVR lead, with the goal of making the diagnosis more rapidly 3. They should also be analyzed in this order.
Vereckei Criteria for VT
If any criteria are met, it is ventricular tachycardia.
- 1. The presence of an initial R wave in lead aVR.
- 2. Width of an initial r wave or q wave >40 ms (one small square).
- 3. Notching on the initial downstroke of a predominantly negative QRS complex.
- 4. Ventricular activation–velocity ratio (vi/vt) <1; vi/vt is the vertical excursion (in millivolts) recorded during the initial (vi) and terminal (vt) 40 ms of the QRS complex.
If none of those criteria are met, it is supraventricular tachycardia.
This algorithm is accurate, reasonably fast, and easy due to the total elimination of complicated traditional morphologic criteria and the simple requirement to evaluate only lead aVR 3.
Other Ventricular Tachycardia Data
There is other data that helps us diagnose ventricular tachycardia.
- Presence of capture beats or fusion beats.
- Ventricular/atrial ratio >1 (more QRS complexes than P waves).
- Heart axis between -90º and -180º (extreme axis deviation).
Referencias
- 1. Wellens HJ, Bar FW, Lie KI. The value of the electrocardiogram in the differential diagnosis of a tachycardia with a widened QRS complex. Am J Med 1978;64:27-33. doi: 10.1016/0002-9343(78)90176-6
- 2. Brugada P, Brugada J, Mout L, Smeets J, Andries EW. A new aproach to the differential
diagnosis of a regular tachycardia with a wide QRS complex. Circulation 1991;83:1649-59. doi: 10.1161/01.CIR.83.5.1649
- 3. Vereckei A, Duray G, Szenasi G, Altemose GT, Miller JM. New algorithm using only lead aVR for differential diagnosis of wide QRS complex tachycardia. Heart Rhythm 2008;5:89-98. doi: 10.1016/j.hrthm.2007.09.020.
- 4. Alzand BSN, Crijns HJGM. Diagnostic criteria of broad QRS complex tachycardia: decades of evolution. Europace . EP Europace 2011;13(4): 465-472. doi: 10.1093/europace/euq430
Si te ha gustado... Compártelo.