As discussed on the article about bundle branch blocks, the bundle of His divides into the right and the left bundle branches.
The complete right bundle branch block (RBBB) occurs when the right branch is not able to conduct the electrical stimulus. Therefore, the depolarization of both ventricles is performed by the left branch.
The electrical stimulus travels down the left branch. First depolarized the left ventricle and the left two-thirds of the septum. Then, with delay, the regions of the right branch are depolarized.
This delay in depolarization causes a widening of the QRS complex.
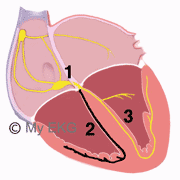
Right Bundle Branch Block
- 1. AV node and bundle of His.
- 2. Blocked right bundle branch.
- 3. Normal left bundle branch.
Electrocardiogram of Complete Right Bundle Branch Block
Electrocardiogram characteristics of right bundle branch block reflect the intraventricular conduction disturbances.
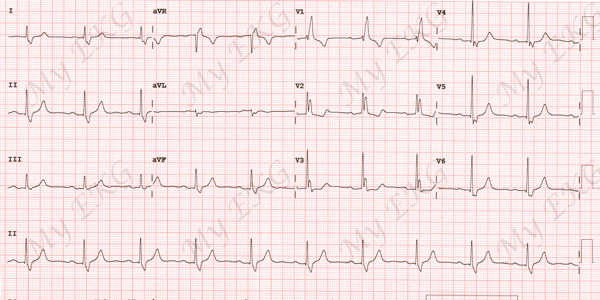
Right bundle branch block:
Wide QRS complex (>120 ms) with rsR’ pattern (wide R’ wave) in lead I, and wide S wave in lead V6.
EKG Criteria of Complete Right Bundle Branch Block
- QRS complex duration greater than or equal to 120 ms in adults, greater than 100 ms in children ages 4 to 16 years, and greater than 90 ms in children less than 4 years of age.
- rsr', rsR', or rSR' pattern in leads V1 or V2. The R' or r' wave is usually wider than the initial R wave. In a minority of patients, a wide and often notched R wave pattern may be seen in lead V1 and/or V2.
- S wave of greater duration than R wave or greater than 40 ms in leads I and V6 in adults.
- Normal R peak time in leads V5 and V6 but greater than 50 ms in lead V1.
Of the above criteria, the first 3 should be present to make the diagnosis. When a pure dominant R wave with or without a notch is present in lead V1, criterion 4 should be satisfied.
Differences Between Normal Conduction and Right Bundle Branch Block
Normal conduction:
The interventricular septum is the first area to be depolarized. On the EKG it is observed as a small initial r wave in V1, and a small initial q wave in V6.
After, the depolarization spreads to both ventricles, with a predominance of the left ventricle, producing a deep S wave in V1 and a tall R wave in V6.
Right Bundle Branch Block:
In right bundle branch block, the beginning of depolarization is similar. Disturbances occur at the end of QRS.
The beginning of the QRS complex is equal to normal, (rS in V1 and qR in V6). But instead of ending, delayed right ventricular depolarization occurs, producing at the end of the QRS, a new R wave (R’) in V1 and a wide S wave in V6.
Differences between Normal EKG and EKG of Right Bundle Branch Block
Normal electrocardiogram: narrow QRS complex. Lead V1 shows an rS pattern and lead V6 shows a qR pattern. T wave is normal.
Electrocardiogram with right bundle branch block: wide QRS complex (>120 ms). Lead V1 shows an rSR’ pattern (broad R’ wave) and lead V6 shows a qRS pattern (broad S wave).
Abnormal depolarization of both ventricles also causes abnormal repolarization. T wave inversions in V1 and V2 are a characteristic finding in right bundle branch block. T waves are positive in leads V4 to V6.
Tip: In right bundle branch block, ST-segment and T wave are deflected opposite the majority of the QRS complex (appropriate T wave discordance).
Treatment of Right Bundle Branch Block
Patients with right bundle branch block without associated heart don't need treatment.
Patients who have right bundle branch block along with another heart condition, treatment of the heart condition is recommended.
The association of right bundle branch block and left fascicular block may present a higher risk of complete AV block (read bifascicular blocks).
Permanent pacemaker implantation is indicated for alternating bundle branch block (RBBB alternating with left bundle branch block)2 3.




