Hypercalcemia on the Electrocardiogram
Hypercalcemia is defined as an increase in the serum calcium level in the plasma higher than 10.4 mg/dL (2.60 mmol/L or 5.2 mEq/L).
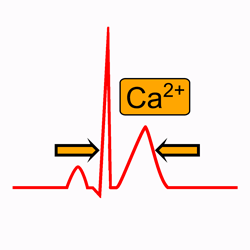
Hypercalcemia may cause electrocardiogram changes, predominantly in the duration of the ST segment and the QT interval, due to alterations in the duration of the plateau of the action potential.
Pathophysiology of Hypercalcemia
Almost all the calcium in the body (99%) is stored in the bone, with only about 1% in the extracellular fluid and 0.1% in the intracellular fluid 1.
About 50% of the total calcium in the plasma exists in the ionized form, which is the form that has biological activity at cell membranes.
The remainder is either bound to the plasma proteins (about 40%) or complexed in the non-ionized form with anions such as phosphate and citrate (about 10%) 1.
Changes in extracellular calcium concentration have a profound effect on the duration of the plateau (phase 2) of the action potential. The duration of the plateau increases at low calcium concentrations and shortens at high calcium concentrations 2.
Because the plateau duration of the ventricular action potential determines the duration of the ST segment, the changes in calcium concentration predominantly affect the duration of the ST segment and thereby the duration of the QT interval 2.
Causes of Hypercalcemia
- Primary hyperparathyroidism
- Familial hypocalciuric hypercalcemia
- Williams syndrome. Idiopathic infantile hypercalcemia
- Secondary hyperparathyroidism:
- Advanced chronic kidney desease
- Tertiary hyperparathyroidism:
- Long-standing secondary hyperparathyroidism
- Patients with end-stage renal disease of several years’ duration.
- Cancer:
- Humoral hypercalcemia: squamous cell carcinoma, renal cell carcinoma, breast cancer, prostate cancer, and ovarian cancer)
- Osteolytic hypercalcemia: metastatic solid tumors (eg, breast, prostate, non-small cell lung cancers) or multiple myeloma, certain lymphomas and lymphosarcomas.
- Ectopic production of calcitriol (lymphoma).
- Vitamin D toxicity
- Granulomatous disorders: sarcoidosis, tuberculosis, leprosy, berylliosis, histoplasmosis and coccidioidomycosis.
- Milk-alkali syndrome: excessive amounts of calcium and absorbable alkali are ingested, usually during self-treatment with calcium carbonate.
Hypercalcemia Definitions:
Normal serum calcium levels are between 8.8 mg/dL (2.1 mmol/L) and 10.4 mg/dL (2.6 mmol/L). Levels above 10.4 mg/dL (2.6 mmol/L) indicate hypercalcemia.
- Mild hypercalcemia: serum calcium between 10.4 mg/dL (2.60 mmol/L) and 11.5 mg/dL (2.88 mmol/L).
- Moderate hypercalcemia: serum calcium between 11.5 mg/dL (2.88 mmol/L) and 18 mg/dL (4.51 mmol/L).
- Severe Hypercalcemia: serum calcium >18 mg/dL (4.50 mmol/L)
Electrocardiogram and Hypercalcemia
In hypercalcemia, the ST segment is short or absent and the duration of the corrected QT interval (QTc) is decreased 2.
The QTc interval is inversely proportional to the serum calcium level up to 16 mg/dL(4 mmol/L) 3.
With marked hypercalcemia, the T wave appears to take off right from the end of the QRS complex 4.
No changes in the QRS and PR durations have been reported.
Hypercalcemia usually does not alter the morphology of the P waves or T waves, but a slight, statistically significant increase in T wave duration was reported.
The U wave amplitude is either normal or increased.
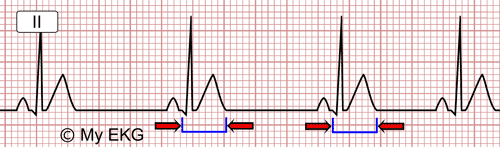
EKG of hypercalcemia: short ST segment and short QTc interval (QTc 285 ms).
In the presence of hypercalcemia associated with hypokalemia, a short QT interval with increased U wave amplitude results in a distinct pattern, most often seen in patients with multiple myeloma.
In severe hypercalcemia, Osborn waves (J waves) may be seen. Severe hypercalcemia may also mimic a ST-segment elevation myocardial infarction on the EKG.
Arrhythmias are uncommon in patients with hypercalcemia. However, sudden death during hyperparathyroid crisis and other conditions associated with severe hypercalcemia may be caused by ventricular fibrillation 2.
Second or third degree AV blocks have been also reported in patients with severe hypercalcemia 2.
Treatment of Hypercalcemia
Treatment of hypercalcemia depends on the severity of symptoms and the underlying cause.
Asymptomatic or mildly symptomatic patients with mild or chronic moderate hypercalcemia may not require immediate treatment 5.
Patients with hypercalcemia of malignancy are typically symptomatic and have markedly elevated calcium levels. These patients will generally need to be managed with urgency, and hypercalcemia of malignancy in many cases represents an oncologic emergency 5.
Mild Hypercalcemia:
Patients with asymptomatic or mildly symptomatic hypercalcemia do not require immediate treatment. Adequate hydration (at least 1.5 to 2 liters of water per day) is recommended.
However, they should be advised to avoid factors that can aggravate hypercalcemia, including thiazide diuretics and lithium carbonate therapy, volume depletion, prolonged bed rest, and a high calcium diet.
Moderate Hypercalcemia:
Asymptomatic or mildly symptomatic individuals with chronic moderate hypercalcemia may not require immediate therapy.
However, an acute rise to these levels may cause gastrointestinal side effects and changes in sensorium, which requires treatment as described for severe hypercalcemia 5.
Severe Hyperkalemia:
Patients with severe hypercalcemia are dehydrated by default and require saline hydration as initial therapy 6.
For immediate short-term management of severe hypercalcemia who are also symptomatic, administration of calcitonin should be considered 5 6.
For longer-term control of hypercalcemia due to excessive bone resorption, is recommend the addition of a bisphosphonate. Denosumab, human monoclonal antibody, is an option for patients with hypercalcemia that is refractory to bisphosphonates 5 6.
Glucocorticoids are effective in treating hypercalcemia due to some lymphomas, sarcoid, or other granulomatous diseases.
Dialysis is considered treatments of last resort. It may be indicated in patients with severe malignancy-associated hypercalcemia and renal insufficiency or heart failure, in whom hydration cannot be safely administered.
Summary
Patients with hypercalcemia typically have a shortened ST segment and a shortened QT interval on the electrocardiogram.
The QTc interval usually is inversely proportional to the serum calcium level, and with marked hypercalcemia, the T wave appears to take off right from the end of the QRS complex.
Management of hypercalcemia includes IV hydration, calcitonin, bisphosphonates, denosumab, and prednisone. Patients with advanced kidney disease and refractory severe hypercalcemia should be considered for dialysis.
We hope this article help you to identify hypercalcemia on the electrocardiogram
Related articles: Hypocalcemia, hyperkalemia, ST segment.
References
If you Like it... Share it.