Hyperkalemia on the Electrocardiogram
Hyperkalemia is an elevated concentration of the serum potassium higher than 5.5 mEq/L.
Hyperkalemia normally cause characteristic changes on the electrocardiogram, which are of vital importance to ensure a quick diagnosis and to estimate the the severity of the hyperkalemia.
Severe hyperkalemia is a life-threatening medical condition, for this reason, it is important to recognize its electrocardiographic findings .
Serum Potassium
About 98% of the total body potassium is found inside cells, and the remaining 2% is in the extracellular space.
High levels of serum potassium cause cardiac conduction system disturbances, producing alterations in the generation and transmission of the electrical stimulus.
Hyperkalemia decrease the resting membrane potential of cardiac myocytes and therefore partially depolarize the cell membrane. This change decreases cardiac contractility and can cause ventricular arrhythmias 1.
The most common causes of hyperkalemia are kidney failure and treatment with ACEi, ARBs or potassium-sparing diuretics. Also can result from other disturbances such as metabolic acidosis, primary Addison syndrome, extensive cell damage (burns, trauma...), among others.
Hyperkalemia Definitions:
Normal serum potassium levels are between 3.5 mEq/L and 5.0 mEq/L. Levels above 5.5 mEq/L indicate hyperkalemia.
- Mild hyperkalemia: Serum potassium between 5.5 mEq/L and 6.5 mEq/L.
- Moderate hyperkalemia: Serum potassium between 6.5 mEq/L and 8.0 mEq/L.
- Severe hyperkalemia: Serum potassium >8.0 mEq/L.
Electrocardiogram and Hyperkalemia
EKG should be done on patients with suspected hyperkalemia or high potassium levels in a blood test in order to determine the severity of hyperkalemia.
The diagnosis of hyperkalemia is usually made by its typical EKG findings.
Severity of Hyperkalemia
Electrocardiogram changes or cardiotoxicity are a determining criterion of severity of hyperkalemia.
Electrocardiogram Findings in Hyperkalemia
In most cases, EKG changes have good correlation with the degree of hyperkalemia. There is a predictable EKG progression as the serum potassium becomes more elevated.
Hyperkalemia is not always expressed with EKG changes. EKG changes also depend on the rate of increase in potassium concentration. Severe hyperkalemia can be seen in absence of classic EKG changes, or severe EKG findings can be seen with potassium levels below 7.0 mEq/L.
Mild Hyperkalemia:
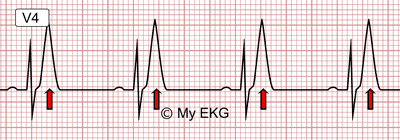
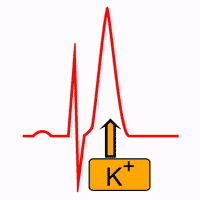
Mild hyperkalemia: Narrow and tall peaked T waves.
Serum potassium between 5.5 mEq/L and 6.5 mEq/L is associated with repolarization abnormalities.
The first and most common change is a progressive increase in the amplitude of the T wave, which becomes tall, thin, narrow-based and peaked “tented”. QT interval may be normal or shortened 2.
Moderate Hyperkalemia:
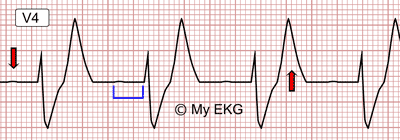
Moderate hyperkalemia: Flattening of the P Wave, prolonged PR interval, widening of the QRS complex and tall T Wave.
Serum potassium level >6.5 mEq/L is associated with disturbance in the whole conduction system (atria, AV node and ventricular branches).
P wave increases in duration and decreases in amplitude, or may disappear. PR and QRS intervals widen with bizarre QRS morphology. T wave remains tall and peaked but is wider.
Other conduction system disorders may appear, such as high-grade atrioventricular blocks, sick sinus syndromes or junctional rhythms.
Severe Hyperkalemia:
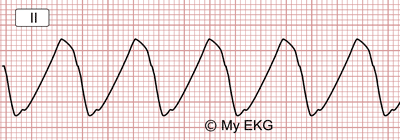
Severe hyperkalemia: Absence of P wave, widened QRS complex with sine-wave morphology.
At serum potassium level >8.0 mEq/L the P wave disappears andthere is a progressive widening of the QRS complex, and the T wave is fused with the QRS obliteration of the ST Segment occurs, culminating in a sine-wave morphology.
This rhythm is a pre-terminal event, can degenerate into ventricular fibrillation or asystole if the cardiac membrane is not stabilized.
Treatment of Hyperkalemia
Treatment of hyperkalemia will depend on the severity of Hyperkalemia.
Mild hyperkalemia: Reducing potassium intake (juices and fruits) and treatment with of Oral Cation exchange resin.
Moderate hyperkalemia: Administration of intravenous rapid insulin (10 UI) plus 25 - 50 g of dextrose. May be given intravenous sodium bicarbonate 1M (if metabolic acidosis), salbutamol 10 - 20 mg via nebulize or 0.5 mg IV, and furosemide IV.
Severe hyperkalemia: Treatment should be started immediately if EKG changes or peripheral neuromuscular abnormalities are present, regardless of the degree of hyperkalemia. In addition to therapeutic measures of moderate hyperkalemia, intravenous calcium gluconate or chloride will be given 3.
The treatment of acute hyperkalemia in end stage renal disease (ESRD) patients is emergent dialysis.
Patients with suspected or known hyperkalemia require IV access and continuous cardiac monitoring.
Summary
Electrocardiogram findings are a determining criterion of severity of Hyperkalemia.
EKG findings generally correlate with the serum potassium level, but potentially life-threatening arrhythmias can occur with normal electrocardiogram.
Narrow and tall peaked T waves are the first sing of hyperkalemia. QRS complex, PR interval and T wave widen, P wave flattens as the serum potassium becomes more elevated.
At serum potassium level >8.0 mEq/L the P wave disappears, the T waves are fused with the QRS complexes culminating in a sine-wave rhythm. This is a life-threatening situation because can degenerate into ventricular fibrillation or asystole.
Ventricular arrhythmias can occur without warning at almost any level of hyperkalemia with normal EKG.
We hope this article help you to identify hyperkalemia in the electrocardiogram.
Related articles: AV blocks, abnormal waves and intervals
References
- 1. Hall JE. Guyton and Hall. Textbook of Medical Physiology. 12th ed. Philadelphia: Elsevier; 2011.
- 2. Mann D, Zipes DP, Libby P et al. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 10th ed. Philadelphia: Elsevier; 2014.
- 3. Alfonzo A, Soar J, MacTie R et al. Treatment of Acute Hyperkalaemia in Adults [Internet]. Renal Association. 2014 [cited: 6 September 2016].
If you Like it... Share it.