Extreme Axis Deviation
Related articles: QRS axis calculation, right-axis deviation, left-axis deviation.
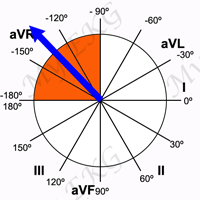
Extreme axis deviation, also known as extreme right axis deviation, northwest axis or “no-man's land” axis, is a rare electrocardiographic finding, and it represents an extreme right- or left-axis deviation 1.
In adults, the normal QRS axis is considered to be within -30° and 90°. Extrem axis deviation is when the QRS axis is between -90° and -180º.
The situations in which extreme axis deviation may be seen are as follows:
Causes of Extreme Axis Deviation
- Misplacement of the limb leads: right arm and left leg leads reversal.
- Ventricular rhythms: ventricular tachycardias, accelerated idioventricular rhythm, ventricular escape rhythm.
- Hyperkalemia.
- Emphysema.
- Ventricular pacing.
Right Arm and Left Leg Leads Reversal
Reversal of the right arm and left leg leads is the most common cause of extreme axis deviation.
When the right arm and left leg leads are reversed, the EKG reveals the following changes 2:
- Lead I is actually upside-down lead III.
- Lead II becomes upside down.
- Lead III is actually upside-down lead I.
- Leads aVR and aVF are reversed.
- Lead aVL is unchanged.
When all the deflections, including the P wave, are negative in lead aVF, a right arm and left leg leads reversal should be suspected 2.
Ventricular Rhythms
Related article: Ventricular arrhythmias.
Ectopic ventricular rhythms (ventricular tachycardias, accelerated idioventricular rhythm or ventricular escape rhythm) arising from the apex of the left ventricle frequently have an extreme axis deviation.
Ventricular Tachycardias
Related article: Ventricular tachycardias.
Ventricular tachycardias are a group of arrhythmias characterized by the presence of three or more consecutive ventricular beats with a high heart rate.
Ventricular tachycardias with right superior axis (extreme axis deviation) usually arise from the apex or septal regions of the left ventricle.
Ventricular tachycardias arising from the apex have right bundle branch block pattern, and ventricular tachycardias adjacent to the left septum have left bundle branch block pattern.
More information: Ventricular tachycardias.
Accelerated Idioventricular Rhythm
Accelerated idioventricular rhythm is an ectopic ventricular rhythm at rates intermediate between escape rhythms and ventricular tachycardias (between 60 and 110 bpm).
This arrhythmia is seen during the first 24 hours in patients with acute myocardial infarction after reperfusion, it indicates a good prognosis.
Ventricular Escape Rhythm
Ventricular escape rhythm is observed on the EKG as a slow, regular rhythm (between 20 and 50 bpm) with wide QRS complexes.
More information: Ventricular arrhythmias.
Hyperkalemia
Related article: Hyperkalemia on the EKG.
An elevation in the plasma potassium concentration >6.5 mEq/L will partially depolarize the cell membrane, producing disorders in the generation and transmission of the electrical stimulus.
Left-axis deviation is the most common axis deviation in hyperkalemia, it is due to a intra-venticular conduction delay, which causes a progressive widening of the QRS complex; but at high serum potassium levels, extreme axis deviation may occur.
More information: Hyperkalemia on the EKG.
Emphysema
Lung hyperexpansion causes external compression of the heart and lowering of the diaphragm, with consequent rotation of the heart in horizontal and frontal planes, this leads to left or right-axis deviation, and in severe emphysema may lead to extreme axis deviation.
In addition, EKG findings of emphysema also include low amplitude of the QRS complexes, right or left QRS axis deviation and P-axis >60° 3.
Ventricular Pacing
When the stimulation site is near the apex of the right ventricle or the apex of the left ventricle, the QRS complex may have extreme axis deviation.
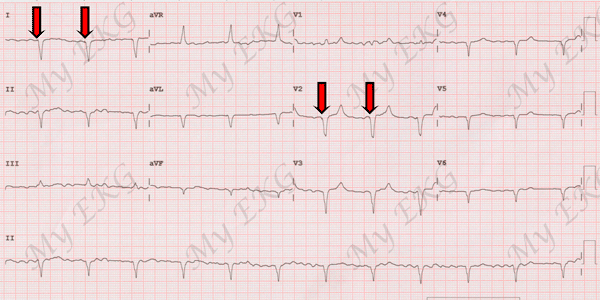
Extreme axis deviation due to ventricular pacing:
QRS axis is about -160º, red arrows indicate the small pacing spikes.
Right ventricular pacing results in QRS complexes similar to those of complete left bundle branch block, and when the stimulation site is in the left ventricle, a complete right bundle branch block pattern is seen.
In most cases of ventricular pacing, the tip of the electrode is located at the apex of the right ventricle.
References
- 1. Surawicz B, Deal BJ et al. AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram Part III: Intraventricular Conduction Disturbances. Journal of the American College of Cardiology Mar 2009, 53 (11) 976-981; DOI: 10.1016/j.jacc.2008.12.013.
- 2. Surawicz B, Knilans TK. Chou’s electrocardiography in clinical practice, 6th ed. Philadelphia: Elservier; 2008.
- 3. Larssen MS, Steine K, Hilde JM, et al. Mechanisms of ECG signs in chronic obstructive pulmonary disease. Open Heart 2017;4:e000552. DOI: 10.1136/openhrt-2016-000552.
If you Like it... Share it.