Hypocalcemia on the Electrocardiogram
Hypocalcemia is defined as calcium level in the plasma below 8.8 mg/dL (2.1 mmol/L or 4.2 mEq/L).
Acute hypocalcemia can be life-threatening, as patients may present with tetany, seizures or cardiac arrhythmias.
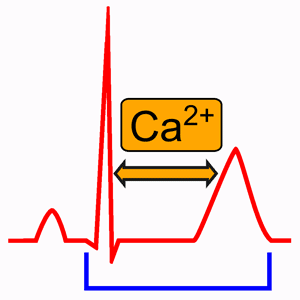
On the electrocardiogram, hypocalcemia may cause a prolongation of the ST segment and the QT interval, due to an increase in the duration of the plateau of the action potential.
Pathophysiology of Hypocalcemia
Almost all the calcium in the body (99%) is stored in the bone, with only about 1% per cent in the extracellular fluid and 0.1% in the intracellular fluid 1.
The calcium in the plasma is present in three forms. About 41% of the calcium is combined with the plasma proteins. About 9% is combined with anionic substances of the plasma and interstitial fluids (citrate and phosphate).
The remaining 50% of the calcium is ionized. This ionic calcium is the form that is important for most functions of calcium in the body, including the effect of calcium on the heart, the nervous system, and bone formation 1.
When serum calcium concentration falls to low levels, the excitability of nerve and muscle cells increases markedly and at concentrations about 50% below may cause hypocalcemic tetany. It also occasionally causes seizures because of its action of increasing excitability in the brain 1.
Hypocalcemia increases the duration of the plateau (phase 2) of the action potential 2.
Because the duration of the plateau of the action potential determines the duration of the ST segment, in the presence of hypocalcemia, the ST segment and the QTc interval are prolonged 2.
Causes of Hypocalcemia
- Hypoparathyroidism
- Postoperative or past radiation
- Autoimmune
- Congenital
- Pseudohypoparathyroidism or pseudopseudohypoparathyroidism
- Hypomagnesemia or severe hypermagnesemia
- Deficiency of vitamin D or vitamin D resistance
- Renal disease or end-stage liver disease causing vitamin D inadequacy
- Hyperphosphatemia
- Acute pancreatitis
- Hungry bone syndrome postparathyroidectomy
- Chelation
- Septic shock or critical illness
- Chemotherapy
- Drugs (eg, phenobarbital, high-dose intravenous bisphosphonates)
Electrocardiogram and Hypocalcemia
In the presence of hypocalcemia, the ST segment and the QTc interval are prolonged. The duration of the ST segment is inversely related to the plasma calcium concentration 2.
Usually lengthening of the ST segment and the QT interval are the only EKG abnormalities in hypocalcemia.
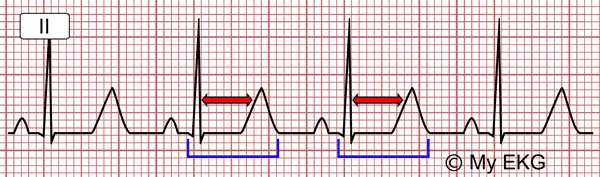
EKG of Hypocalcemia: prolonged ST segment and prolonged QTc interval (QTc 537 ms).
Hypocalcemia usually can be recognized on the EKG because, with the possible exception of hypothermia, there are no other agents or metabolic abnormalities that prolong the duration of the ST segment without changing the duration of the T wave.
Note, however, that patients may have clinically significant hypocalcemia without diagnostic EKG changes 3.
In the presence of hypocalcemia, the polarity of the T wave may remain unchanged. Sometimes, however, the T wave becomes low, flat, or sharply inverted in leads with an upright QRS complex 2.
In patients with a prolonged QT interval due to hypocalcemia, the U wave is usually absent or not recognizable 2.
Treatment of Hypocalcemia
Treatment of hypocalcemia depends on the severity of symptoms, the underlying cause, and how rapidly the hypocalcemia developed.
All treatment requires close monitoring. If intravenous infusions are contemplated, hospitalization in an intensive care unit or specialized unit with access to cardiac monitoring and rapid ionized calcium determinations is ideal for optimal management and safety.
Acute Hypocalcemia:
Acute hypocalcemia can be life-threatening. Patients with acute symptomatic hypocalcemia or calcium level lower than 7.0 mg/dL (1.75 mmol/L) should be treated promptly with IV calcium 4 5.
Calcium gluconate is preferred over calcium chloride because it causes less tissue necrosis if extravasated.
100 to 200 mg of elemental calcium diluted in 50 to 100 mL of 5% dextrose should be given over 10 to 20 minutes (calcium gluconate contains 90 mg of elemental calcium per 10 mL) 4 5.
Rapid administration could result in arrhythmias so intravenous administration should be carefully monitored.
It is essential to measure serum magnesium in any patient who has is hypocalcemia, coexisting hypomagnesemia should be corrected 4 5.
Chronic Hypocalcemia:
Oral repletion may be indicated for asymptomatic or mildly symptomatic patients. If this is insufficient, vitamin D supplementation should be added 4 5.
Serum calcium should be tested every 3 to 6 months or when any changes in the medical regimen are made. The serum calcium level should be targeted to about 8.0 mg/dL (2.0 mmol/L).
One potential side effect is hypercalciuria which can be complicated by nephrocalcinosis, nephrolithiasis, and or renal insufficiency.
Thiazide diuretics can increase renal calcium reabsorption, if hypercalciuria is detected, a thiazide diuretic may be added.
Furosemide and other loop diuretics can depress serum calcium levels and should be avoided.
Recombinant human PTH was approved in 2015 for the treatment of hypoparathyroidism in patients not well controlled on therapy with calcium supplements and vitamin D.
Summary
Patients with acute hypocalcemia may present tetany, seizures or cardiac arrhythmias.
In the presence of hypocalcemia, the ST segment and the QTc interval are prolonged.
The duration of the ST segment is inversely related to the plasma calcium concentration.
Treatment of hypocalcemia depends on the severity of symptoms, the underlying conditions, and how rapidly the hypocalcemia developed.
We hope this article help you to identify hypocalcemia on the electrocardiogram.
Related articles: Hypercalcemia, hyperkalemia, ST segment.
References
- 1. Hall JE. Guyton and Hall. Textbook of Medical Physiology. 12th ed. Philadelphia: Elsevier; 2011.
- 2. Surawicz B, Knilans TK. Chou’s electrocardiography in clinical practice, 6th ed. Philadelphia: Elservier; 2008.
- 3. Goldberger A. Clinical Electrocardiography: A Simplified Approach. 7a ed. Philadelphia: Mosby Elsevier; 2006.
- 4. Schafer AL, Dolores M Shoback, DM. Hypocalcemia: Diagnosis and Treatment. Endotext [Internet]. 2016 [cited: March 29, 2016].
- 5. Skugor M. Hypocalcemia. Cleveland Clinic [Internet]. 2014 [cited: March 29, 2016].
If you Like it... Share it.