Right Axis Deviation
Related articles: Heart axis calculation, left-axis deviation, extreme axis deviation.
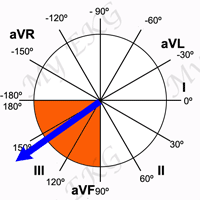
In adults, the normal QRS axis is considered to be within −30° and 90°, right-axis deviation is considered from 90° to 180º 1.
Moderate right-axis deviation is from 90° to 120°, and marked right-axis deviation, which is often associated with left posterior fascicular block, is between 120° and 180° 2.
The situations in which right-axis deviation may be seen are as follows:
Causes of Right Axis Deviation
- Normal variation (e.g., children, young or slender adults).
- Left and right arm leads reversal.
- Left posterior fascicular block.
- Right ventricular hypertrophy.
- Lateral wall myocardial infarction.
- Acute or chronic lung diseases: pulmonary embolism, pulmonary hypertension, chronic obstructive pulmonary disease (COPD), cor pulmonale.
- Congenital heart disease (e.g., dextrocardia, tetralogy of Fallot, transposition of the great arteries, atrial and ventricular septal defects).
- Wolff-Parkinson-White syndrome.
- Ventricular ectopic rhythms (e.g., ventricular tachycardia).
Normal Variation
Right-axis deviation occurs normally in infants and children 3 (read pediatric EKG). At birth, the mean QRS axis lies between 60° and 160°. By age 1 year, the axis changes gradually to lie between 10° and 100° 4.
In the adult population, tall and slender subjects tend to have a rightward QRS axis 3.
Left and Right Arm Leads Reversal
Reversal of the arm leads is the most common lead placement error.
It is the easiest to recognize because of a negative P wave in lead I in patients with sinus rhythm, which is unusual even in the presence of heart disease 3.
Left and right arm leads reversal:
Negative P wave in lead I. Lead I is upside down. Lead II is actually lead III and vice versa. Lead aVR is actually lead aVL and vice versa.
When the left and right arm leads are reversed, the EKG reveals the following changes:
- Negative P wave in lead I.
- Lead I is upside down because the polarity of the lead is reversed.
- Lead II is actually lead III and vice versa.
- Lead aVR is actually lead aVL and vice versa.
In patients with atrial fibrillation or unidentifiable P waves, the morphology of the ventricular complexes in leads I, V5, and V6 should be similar.
If the polarity of the QRS complex in lead I is opposite that in the left precordial leads, arm lead reversal should be suspected 3.
Left Posterior Fascicular Block
Related article: Left fascicular blocks.
In left posterior fascicular block there is a delay in the activation of the posterior region of the left ventricle, which produces a marked right-axis deviation (120º or more), without widening of QRS complex.
It also causes a rS pattern in leads I and aVL and a qR pattern in leads III and aVF 2.
More information: Left fascicular blocks.
Right Ventricular Hypertrophy
Related article: Right ventricular hypertrophy.
Right ventricular hypertrophy (RVH) causes a displacement of the QRS vector toward the right and anteriorly and often causes a delay in the R wave peak in right precordial leads 5.
Electrocardiographic RVH has often been classified on the basis of two EKG patterns 3 5:
One pattern consists of predominantly tall R waves (Rs, R, or Qr pattern) in right precordial leads (typical RVH pattern) 3, and second pattern consists of incomplete right bundle branch block, suggesting volume overload 5.
Both patterns are associated with right-axis deviation.
More information: Right ventricular hypertrophy.
Lateral Myocardial Infarction
In patients with lateral myocardial infarction, the loss of leftward forces may result in a rightward shift of the QRS vector.
In these patients the initial R wave in lead I is usually absent, however, and abnormal Q waves are often observed also in the left precordial leads.
Inverted T waves in leads I, aVL, V5, and V6 may also be present in patients with lateral myocardial infarction.
Chronic Obstructive Pulmonary Disease (COPD)
The characteristic EKG pattern in patients with chronic obstructive pulmonary disease (COPD) is attributed to changes in the spatial orientation of the heart, the insulating effect of the overaerated lungs, and the low position of the diaphragm.
Typical EKG changes of COPD include peaked P waves in inferior leads (II, III, and aVF), persistent S waves in all precordial leads, low R wave amplitude in all leads, and a frontal plane QRS axis that is rightward, superior, or indeterminate.
Pulmonary Embolism
Related article: Pulmonary embolism.
Pulmonary embolism may cause right-axis deviation, incomplete or complete right bundle branch block, or EKG signs of right ventricular overload (negative T waves in leads V1-V4, McGinn-White sign or S1Q3T3 pattern).
The electrocardiogram is not a sensitive test for the diagnosis of pulmonary embolism. The most frequent EKG finding in pulmonary embolism is sinus tachycardia.
More information: Pulmonary embolism.
Other Causes of Right Axis Deviation
Abnormalities of axis are rarely specific in the diagnosis of congenital heart diseases. Tetralogy of Fallot, transposition of the great arteries, total anomalous pulmonary venous return, ventricular and atrial septal defect may causes cause right-axis deviation 6.
Right-axis deviation may also be seen in high degrees of pre-excitation or during a ventricular tachycardia.
References
- 1. Mason JW, Hancock EW et al. Recommendations for the Standardization and Interpretation of the Electrocardiogram. Part II: Electrocardiography Diagnostic Statement List A Scientific Statement From the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society Endorsed by the International Society for Computerized Electrocardiology. JACC. 2007; 49(10) 1128-1135. doi: 10.1016/j.jacc.2007.01.025.
- 2. Surawicz B, Deal BJ et al. AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram Part III: Intraventricular Conduction Disturbances. Journal of the American College of Cardiology Mar 2009; 53(11) 976-981. doi: 10.1016/j.jacc.2008.12.013.
- 3. Surawicz B, Knilans TK. Chou’s electrocardiography in clinical practice, 6th ed. Philadelphia: Elservier; 2008.
- 4. Goodacre S, McLeod K. Paediatric electrocardiography. BMJ. 2002; 324: 1382–1385. doi: 10.1136/bmj.324.7350.1382.
- 5. Hancock EW, Deal BJ et al. AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram. Part V: Electrocardiogram Changes Associated With Cardiac Chamber Hypertrophy: A Scientific Statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: Endorsed by the International Society for Computerized Electrocardiology. Circulation. 2009; 119: e251-e261. doi: 10.1161/CIRCULATIONAHA.108.191097.
- 6. O'Connor M, McDaniel N, Brady WJ. The pediatric electrocardiogram Part III: Congenital heart disease and other cardiac syndromes. Am J Emerg Med. 2008 May; 26(4): 497-503. doi: 10.1016/j.ajem.2007.08.004.
If you Like it... Share it.




