Left Axis Deviation
Related articles: Heart axis calculation, right-axis deviation, extreme axis deviation.
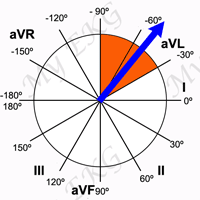
In adults, the normal QRS axis is considered to be within -30° and 90°. Left-axis deviation is when the QRS axis is between -30° and -90º.
Moderate left-axis deviation is between -30° and -45°. Marked left-axis deviation is from -45° to -90° and is often associated with left anterior fascicular block 1.
The situations in which left-axis deviation may be seen are as follows:
Causes of Left Axis Deviation
Note that the first three account for almost 90% of EKG tracings with left-axis deviation.
Normal variation
The mean QRS axis tends to shift leftward with increasing age. The leftward shift of the QRS axis with aging is particularly prevalent in overweight subjects and is more pronounced in older obese men than in older obese women 3.
There is an association between the QRS axis and body weight, overweight individuals tend to have a more leftward axis. Most obese patients without clinical heart disease have normal EKGs, with the mean QRS vector shifting to the left with increasing obesity 3.
Left Ventricular Hypertrophy
Related article: Left ventricular hypertrophy.
In patients with left ventricular hypertrophy, QRS axis may be within normal (but between 0º and -30º) or deviated to the left 2.
The most frequent findings of LVH on the EKG are tall R waves in left precordial leads (V5-V6) and deep S waves in right precordial leads (V1-V2). There is also an increase in QRS complex duration, greater than 100 ms.
It is common to find ST-segment depression and negative T waves in lateral leads (I, aVL, V5 or V6).
Signs of left atrium enlargement may be observed with wide P waves (P mitrale) in inferior and left precordial leads 2.
More information: Left ventricular hypertrophy.
Left Anterior Fascicular Block
Related article: Left fascicular blocks.
In left anterior fascicular block there is a delay in the activation of the anterior region of the left ventricle, which produces a marked left-axis deviation (QRS axis between -45° and -90°), without widening of QRS complex.
It also causes a rS pattern in leads II, III and aVF, and a qR pattern in leads I and aVL 1.
More information: Left fascicular blocks.
Left Bundle Branch Block
Related article: Left bundle branch block.
In left bundle branch block (LBBB), the QRS duration is greater than or equal to 120 ms in adults, there is broad notched or slurred R wave in leads I, aVL, V5 and V6.
The ST-segment and T waves are usually opposed to QRS direction.
The appearance of LBBB may change the mean QRS axis in the frontal plane to the right, to the left, or to a superior, in some cases in a rate-dependent manner 3.
More Information: Left bundle branch block.
Inferior Wall Myocardial Infarction
Inferior wall myocardial infarction is another condition which may lead to abnormal left-axis deviation.
In an inferior myocardial infarction the initial QRS forces are directed superiorly, causing an abnormal Q wave in leads II, III, and aVF.
Inverted T waves in inferior leads (II, III, and aVF) may also be present in patients with inferior myocardial infarction.
Hyperkalemia
Related article: Hyperkalemia on the EKG.
An elevation in the plasma potassium concentration >6.5 mEq/L will partially depolarize the cell membrane, producing disorders in the generation and transmission of the electrical stimulus.
Left-axis deviation that occur in hyperkalemia are due to a intra-venticular conduction delay, which causes a progressive widening of the QRS complex.
P wave also increases in duration and decreases in amplitude and, furthermore, other disorders may appear, such as AV blocks, sick sinus syndromes or junctional rhythms.
More information: Hyperkalemia on the EKG.
Emphysema
Lung hyperexpansion causes external compression of the heart and lowering of the diaphragm, with consequent elongation and vertical orientation of the heart.
In addition, the presence of increased air between the heart and recording electrodes reduces the amplitude of the QRS complexes in precordial leads.
Low voltage in limb leads, right QRS axis deviation (>90°) or left QRS axis deviation (beyond -30°), combined with a P-axis >60°, are reported to be pathognomonic for emphysema 4.
Other Causes of Left Axis Deviation
Abnormalities of axis are rarely specific in the diagnosis of congenital heart diseases. Ostium primum atrial septal defect an atrioventricular canal may causes left-axis deviation 5.
Left-axis deviation may also be seen in high degrees of pre-excitation, during a ventricular tachycardia, in a paced rhythm 2, in expiration, pregnancy, ascites, etc.
References
- 1. Surawicz B, Deal BJ et al. AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram Part III: Intraventricular Conduction Disturbances. Journal of the American College of Cardiology Mar 2009, 53 (11) 976-981; DOI: 10.1016/j.jacc.2008.12.013.
- 2. Kashou AH, Kashou HE. Electrical Axis (Normal, Right Axis Deviation, and Left Axis Deviation) [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan
- 3. Surawicz B, Knilans TK. Chou’s electrocardiography in clinical practice, 6th ed. Philadelphia: Elservier; 2008.
- 4. Larssen MS, Steine K, Hilde JM, et al. Mechanisms of ECG signs in chronic obstructive pulmonary disease. Open Heart 2017;4:e000552. DOI: 10.1136/openhrt-2016-000552.
- 5. O'Connor M, McDaniel N, Brady WJ. The pediatric electrocardiogram Part III: Congenital heart disease and other cardiac syndromes. Am J Emerg Med. 2008 May;26(4):497-503. DOI: 10.1016/j.ajem.2007.08.004.
If you Like it... Share it.