Pediatric Electrocardiogram

Image courtesy of Serge Bertasius Photography / FreeDigitalPhotos.net
The electrocardiogram remains an important test for the diagnosis and evolution of congenital heart disease, arrhythmias or other heart conditions during childhood.
The basic principles of pediatric electrocardiogram are identical to those in adults, but in children, the EKG presents different features, conditioned by the patient's age.
In this article we give you all the tools for correct interpretation of a pediatric EKG and its differences with the adult electrocadiogram.
How to perform an Electrocardiogram to a child?
The electrocardiogram is performed in a child in the same way as adult EKG.
10 electrodes are placed in their usual positions, and should prevent the child from moving during EKG acquisition (this is the hard part).
Limb electrodes can be placed on the torso to reduce movement artifacts.
In newborns and infants must also make V3R and V4R (right-side leads) for a better study of the right ventricle.
When done, it should be reviewed before removing the electrodes, ensuring proper calibration and the absence of artifacts or poorly recorded Leads.
Differences between the Pediatric and Adult Electrocardiogram
The pediatric electrocardiogram has different features, these differences are more pronounced in newborns, and, as the patient grows, are varying through adolescence.
Electrocardiogram of a Newborn:
In newborns there is a predominance of the right ventricle to the left ventricle due to the fetal circulation.
On the EKG trace can be observed:
- Heart rate between 90 and 160 bpm.
- Right-axis deviation (between 70º and 180º).
- Tall R waves in lead V1 and deep S waves in lead V6.
- Shorter waves (P, T) and intervals (PR, QRS).
- Positive T waves in precordial leads at birth, becoming negative in leads V1-V3 after the first week of life.
- Deep Q wave in inferior leads and V5-V6.
Electrocardiogram Changes With Age:
Heart axis: the QRS axis direction is moving toward normal values (between -30º and 90º).
Precordial leads: R wave in lead V1 and S wave in lead V6 are becoming smaller, while S wave in lead V1 and R wave in lead V6 increase their amplitude.
Heart rate: as the child grows, heart rate decreases. In the healthy adult it is between 60 and 100 bpm.
Length of waves and intervals: The length of the waves and intervals of the electrocardiogram increases with age (wider waves and longer intervals).
T wave: T wave is positive in precordial leads in newborns, but after the first week of life becomes negative in leads V1-V3 and persists through adolescence and even, in young adults (juvenile T wave pattern).
For a correct analysis of pediatric EKG it is essential to know the age of the patient and also know the normal values of each age.
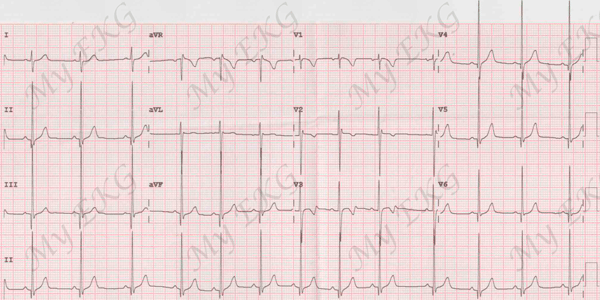
Electrocardiogram from a healthy 2 year old child:
Sinus arrhythmia with heart rate of 76 bpm, negative T waves in leads V1-V3, QRS axis of 90º.
Normal Values of Pediatric Electrocardiogram
The following table shows the normal values for heart rate, heart axis, length of waves and intervals and amplitude of the R waves and S waves in leads V1 and V6 in each pediatric age range.
| Age |
0-7 days |
8-30 days |
1-6 months |
6-12 months |
1-5 years |
5-10 years |
10-15 years |
adult |
| HR (bpm) |
90 - 160 |
100 - 175 |
110 - 180 |
70 - 160 |
65 - 140 |
60 - 130 |
60 - 100 |
| PR (ms) |
80 - 150 |
50 - 150 |
80 - 150 |
90 - 180 |
100 - 200 |
| Eje (º) |
70 - 180 |
45 - 160 |
10 - 120 |
10 - 110 |
5 - 110 |
| QRS (ms) |
40 - 70 |
45 - 80 |
50 - 90 |
60 - 90 |
| QRS V1 (mV) |
| Q |
No Q wave |
| R |
0,5 - 2,5 |
0,3 - 2,0 |
0,2 - 2,0 |
0,2 - 1,8 |
0,1 - 1,5 |
0,1 - 1,2 |
0,1 - 0,6 |
| S |
0 - 2,2 |
0 - 1,6 |
0 - 1,5 |
0,1 - 2,0 |
0,3 - 2,1 |
0,3 - 2,2 |
0,3 - 1,3 |
| T |
-0,3 - 0,3 |
-0,6 to -0,1 |
-0,6 - 2 |
-0,4 - 0,3 |
-0,2 - 0,2 |
| QRS V6 (mV) |
| Q |
0 - 0,2 |
0 - 0,3 |
0 - 0,4 |
0 - 0,3 |
0 - 0,2 |
| R |
0,1 - 1,2 |
0,1 - 1,7 |
0,3 - 2,0 |
0,5 - 2,2 |
0,6 - 2,2 |
0,8 - 2,5 |
0,8 - 2,4 |
0,5 - 1,8 |
| S |
0 - 0,9 |
0 - 0,7 |
0 - 0,6 |
0 - 0,4 |
0 - 0,2 |
Non-pathological Changes of Pediatric Electrocardiogram
In children, is common to find changes in the electrocardiogram which are considered non-pathological disorder.
Sinus arrhythmia: changes in heart rate (PP intervals) with breathing. Sinus arrhythmia occurs often in children, adolescents and young adults. Is considered a normal sinus rhythm variation.
Wandering atrial pacemaker: sinus P waves alternating with ectopic P waves. It is observed as P waves with different morphologies in the same lead. The PR interval may also be variable. Wandering pacemaker is usually caused by increased vagal tone, rarely causes symptoms or requires treatment.
Supraventricular extrasystoles: presence of a narrow premature QRS. It may be preceded by ectopic P wave (atrial origin) or not (node origin). No pathological significance, but may cause symptoms.
RSR’ pattern in V1: the incomplete left bundle branch block is also often found in childhood and youth, in patients without heart disease. Although if it is accompanied by heart murmur, an atrial septal defect should be ruled out.
First degree AV block and second degree AV block, type I (Wenckebach): may be seen in children with increased vagal tone, no pathological significance (see AV blocks).
Early repolarization: concave ST segment elevation with terminal QRS slurring or notching (J wave). It is an EKG pattern most commonly seen in adolescents and young athletes. No pathological significance, although, it has been found to be associated with a modest increased risk of ventricular arrhythmias, in some recent studies (see early repolarization).
If you Like it... Share it.




